It’s been a busy couple of weeks and I have been in a bit of a funk for most of it. I started writing several posts but never published them. I’m just not feeling it, I feel like I have nothing to contribute. I feel like I’m all doom and gloom these days and trying to be positive is just not working. So rather than bore all of you with my mundane drivel I’ve been hanging low.
I have been reading loads of great blogs but I haven’t even really had the opportunity to comment on them, which I would like to do. So I’m going to try to make some time to do that tomorrow. I also drastically need to update my blogroll because I think I am following in the region of 200+ blogs at the moment and they all deserve recognition. I promise to do that soon.
On the upside I had my last day at my old job the other day. I am finally free of the Sweet Pea Thief. And it feels damn good. I immediately felt the huge weight lifted off my shoulders. It could not have come soon enough. The constant drooling over her by others nearly did my head in. I literally sat at my desk with my headphones on max so I didn’t have to hear the crap they were spewing over her. I even managed to skirt my leaving drinks, and saying goodbye to her and the rest of my colleagues because thankfully my last day was spent entirely in meetings and one of my particularly needy clients wanted a handover meeting as the last thing I did that day, which meant I was nowhere near the office on my last day. Couldn’t have worked out better if I had planned it.
I had one day off in between jobs which I spent getting a massage, going to the spa and having lunch with a friend and her brand new puppy who is pretty freaking cute right?

I know, she’s crazy cute. It was a pretty great day. I felt rested and ready for the new job the next day.
And so far the new job is pretty good. Despite a few very stressful days last week when I was kind of working for them while also working for the other place (naughty I know), for the most part it’s going well. It’s always a scary transition isn’t it, but the people and environment are nice and I am busy (in a good way) right away. I have had plenty of “what am I doing” moments but I guess these are to be expected when going through this kind of transition. Being anonymous feels great. No one there knows my story except for a super good friend of mine who started working there this week too. She happens to be one of the most supportive people in real life right now. And I even like my view on my commute home.

Not bad right? So everything seems somewhat positive, I am feeling good about that side of life.
I had my second LIT treatment yesterday. This one was far more painful than the first and my skin bubbled up in hives immediately. This apparently means it’s working. I was far too annoyed to listen to that because I was too busy watching the dumbass nurse eject at least £200 worth of the Hubs white blood cells onto her lap when it was meant for my arm. Stupid stupid fool. Today I’m bandaged up and sore and glad it’s over. I won’t need another one for 6 months or so.
In the meantime, this cycle was pretty much a bust. I felt like it was a bust from the very start. Just wasn’t feeling it. I tested on 9dpo and 11dpo and both were white as snow. So I came off the progesterone support so AF could make her appearance. I’ve been feeling pretty crampy and emotional and was just riding it out for AF. I was actually OK at processing the disappointment this month. On one hand I felt slightly relieved because next cycle I would officially qualify for maternity pay should I be lucky enough to fall pregnant again, but on the other hand it was yet another sad result. I had a good cry that evening and felt a bit out of sorts but was already looking ahead at what I would do differently for next cycle.
Viagra suppositories. Yep, my womb lining needs all the help it can get and a few of those puppies can do a girl’s lining wonders. I was poised on “click to buy” online when I decided to do one more test this morning for the hell of it, purely because Viagra is expensive and I don’t want to be out of pocket for something I might not need for a while. Anyway, I was confused as to why AF is still nowhere to be seen when my cramps have been pretty full fledged for 5 days now. AF is only one day late but this is not unusual, especially after last cycle’s trauma.
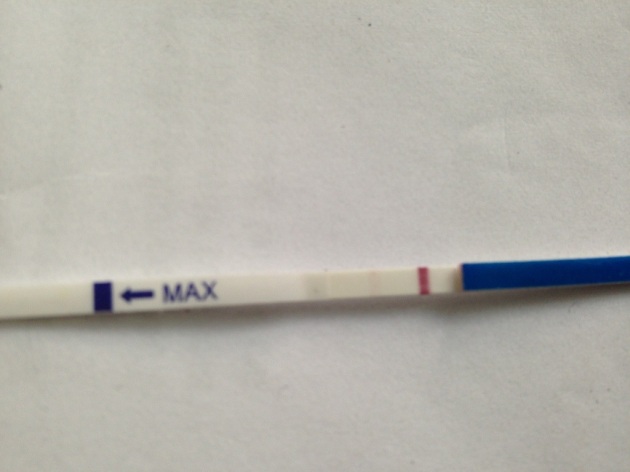
Today is 15dpo. Sorry for the shit pic but can you see a second line? Because I can barely see a second line. In fact, I totally missed this second line. First thing this morning after I peed on this stick and saw within thirty seconds that it was stark white, I went back to bed. It was only a few hours later when I was having a pee when I glanced over at it and saw a super faint not even really there second line. Convinced this was an evaporation line, I quickly sought the advice of Doctor Google who says that an evaporation line is a different colour to the test line. This second line is pink. Pink like the test line.
Commence freak out. I had been really successful at ignoring any symptoms and not allowing any symptom spotting to occur during the 2WW this cycle. That is, until my telltale symptom kicked in. The raging super quick pulse I get in my abdomen. This has only ever meant one thing. And when the pulsating hum hadn’t stopped this morning I ran out to buy a digital test expecting it to be negative. Instead I got this.

I’m sad to admit it but we didn’t even smile for each other. There were no hugs or high fives or elated kisses. Instead we muttered a few “oh dears” and sat in silent shock at the result sitting before us. What the hell do we do now.
A faint positive at 15dpo is considered late implantation. Consistently, the last five pregnancies have all been late implanters. All five pregnancies ended in tears. This has been a critical part of my diagnosis with the unfortunately termed condition known as “super fertility.” I know all too well what a faint double line means at this late stage. I have been off progesterone for four days now so who knows what havoc this has caused for my lining or for the poor little embie trying to make a home.
I could list all the things that I have done wrong in these two weeks. For someone who is acutely aware of what to do and not to do in the 2WW I have been pretty lame at it this cycle. My gloom got the better of me. Because I expected things to fail this cycle I lived like they had. I could have stayed on the progesterone, and messed up my cycle for a few more days but provide the support the embie needs. I could have not gone to the spa or spent all day getting hot, then cold, then hot, then cold. I could have eaten better or slept when I needed it or gone on the steroids I’ve been prescribed but been too reluctant to go on. But there is nothing I can do about any of that now.
But I guess on the flipside there are a lot of things we have done differently this time around. Since our last loss I’ve been diagnosed with a clotting disorder, immune issues and a defective womb. And we are / will be actively treating all these things. Aspirin, progesterone, LIT, intralipids, clexane, prednisone, chinese herbs, acupuncture. We can only hope that one / all of these treatments might tip the scales this time.
I am angry that a moment that should be full of happiness and celebration was replaced with impending doom, fear and raw panic. How can I stop feeling this way? How can I turn this around? How does one do that exactly?
Will history repeat itself? I don’t know. There is nothing I can do to change the outcome of this. All I can do is try to look forward. Try to be hopeful. Try to take one step a time. The phrase has never been more poignant in all my life.





